
A neurobiologist looks at the death penalty cocktail
This week, neurobiology bumped up into current events and it all played out in the context of teaching. I taught a module on Neural Communication to my second year Pritzker Medical School students. One of the topics that I covered is how neurons understand the message that is sent their way, a lecture that centers on post-synaptic receptors and the drugs that act on them. Given that there are >1000 receptors that decorate neuronal dendrites, I obviously pare down the group to a “greatest hits” group. Among the star-receptors featured is the nicotinic acetylcholine receptor (nAChR). To imbue the nAChR with some character and interest, I tell the students of native South American tribes that used curare-dipped arrows to incapacitate prey. Curare acts as a nAChR antagonist, blocking motoneurons from effectively communicating with skeletal muscle, and thereby “relaxing” the muscles. I then tell the students of pancuronium, another nAChR antagonist that also acts as a muscle relaxant. Beyond its extreme utility as a muscle relaxant during surgery, I mention that pancuronium has long been used by states within the U.S. as one of the drugs administered to prisoners condemned to die by lethal injection.
After talking about nAChRs, I go on to talk about GABAA receptors, which are pharmacological treasure troves. Drugs that act on these receptors include anxiolytics (e.g. Xanax), hypnotics (e.g. Ambien), anticonvulsants (e.g. Klonopin), and general anesthetics (including propofol, Forane, and barbiturates). Obviously the GABAA receptor is very important in clinical medicine. But it is also important in governmentally mandated executions. General anesthetics, which greatly facilitate communication via the GABAA receptor, were part of the pharmacological attack used to intentionally kill people. Twenty years ago, prisoners slated to be killed by the state would receive a cocktail of three drugs:
- A barbiturate general anesthetic that induces unconsciousness rapidly (typically sodium thiopental). This unconsciousness lasts for hours but, at the doses used, is not in and of itself lethal.
- Pancuronium serves as a muscle relaxant. This prevents breathing (dependent on the diaphragm muscle) and also opposes twitches or more substantial movements of the limbs or facial muscles. This muscle relaxation would slowly deprive a person of oxygen, resulting eventually in cardiac cessation as well.
- Potassium chloride (KCl) is used as a source of excessive potassium ions that paralyzes the heart muscle and rapidly brings about asystole. This is a fancy way of saying that very shortly after a correct dose of KCl is administered, the heart stops beating.
Fast forward 15 years or so and the picture is different in legal and pharmaceutical ways. On the legal front, several U.S. states, including Illinois where I reside, have abolished the death penalty. After three decades when a total of three jurisdictions (MA, RI, & DC) abolished the death penalty, seven (NJ, NY, NM, IL, CT, MD & Nebraska) have done so in the last nine years. While 31 states still have the legal right to put prisoners to death, less than half of these states, 14 to be exact, have in fact killed a prisoner in the last 5 years and more than a third of the 183 prisoners killed by a U.S. state between 2011 and today were killed by the state of Texas. State-mandated killing, after reaching a peak in popularity just before the turn of the millennium, appears to be declining in popularity.
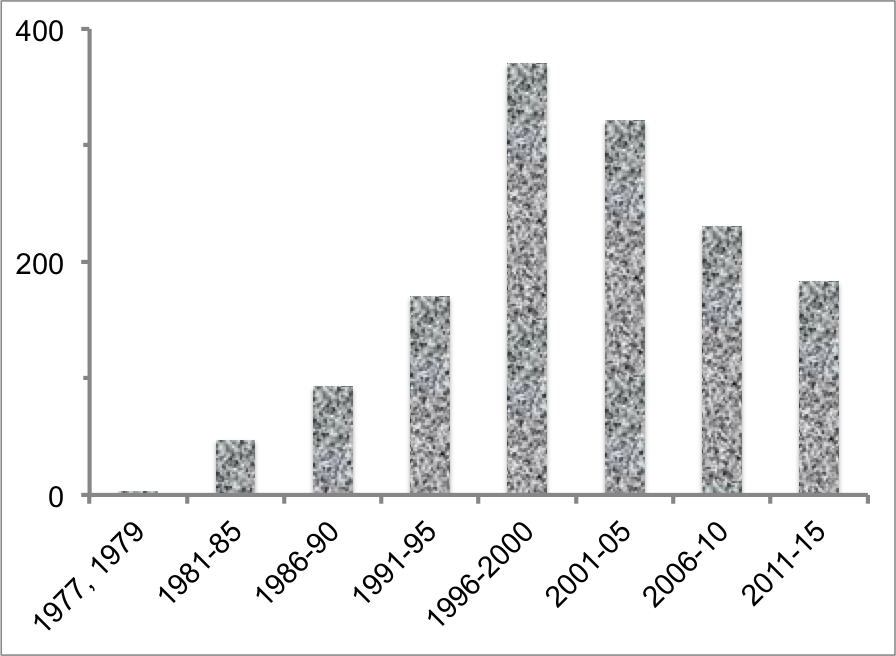
The number of executions that have taken place in the United States since the 1976 Gregg v. Georgia decision of the Supreme Court. Six more prisoners are currently scheduled to be executed by Texas (4), Florida (1), and Montana (1) in 2015. Data are from the Death Penalty Information Center.
Let’s return to pharmacology. Problems with lethal injection arose in the noughts, 2000-2009. The European Union strongly opposes the death penalty. It is my understanding that the E.U. placed pressure on pharmacological companies that were providing the drugs that U.S. states were using to kill and that in particular, the E.U. targeted the sale of barbiturates. There would be no motivation in trying to ban traffic in potassium chloride (KCl), a common chemical with a myriad of commercial uses, or pancuronium, a drug of huge clinical utility. But barbiturates are different as demand has greatly decreased since general anesthetics better suited to clinical use have been developed.
The above story highlighting a role for the E.U. in making sodium thiopental impossible to get in the U.S. may not be correct. I strongly recommend that those interested in this history read the piece by Jeffrey E Stern in the The Atlantic. While not focused on the history of barbiturate availability, this journalistic gem does suggest that the FDA was also instrumental in making barbiturates difficult to obtain in the U.S.
Regardless of how it came about, the supply of barbiturates for lethal injection did dry up, and at this point, U.S. states made a curious decision. They started to use midazolam (aka Versed) in place of sodium thiopental (or sodium pentobarbital, another barbiturate). This is a curious curious choice because midazolam and sodium thiopental are not even members of the same class and do not accomplish the same end. Midazolam is a benzodiazepine that serves as an anxiolytic. Sodium thiopental is a general anesthetic that causes deep unconsciousness. What I learned from Mr. Stern’s article is that these facts would not have been known to the individuals tasked with obtaining the drugs, who were lawyers, wardens, correctional officers and the like. They were not health professionals (which makes some sense since there is nothing health-related in executions).
Florida, Ohio and Oklahoma plunged ahead with a new cocktail in which midazolam replaced sodium thiopental. Since this cocktail lacked a general anesthetic, it was not effective and prisoners experienced a prolonged agonal period without being knocked out. The prisoners moaned, spoke, and made purposeful movements for minutes to hours as they slowly died. In the case of Clayton Lockett, the problems with the cocktail were greatly exacerbated by prolonged incompetence on the part of a paramedic and a physician who could not place an intravenous catheter in the prisoner, resulting in the drugs acting very, very slowly. As Mr. Stern writes in his gripping must-read piece, a lawyer for Mr Lockett said that what happened to Mr. Lockett can only be characterized as “human experimentation.”
What is going on here? Well, midazolam does not make a person unconscious. This is not so evident in the absence of noxious stimulus when a midazolam-treated person may well remain very sedated. However, in the presence of noxious stimulation, the perceived pain breaks through the midazolam sedation. The reader may be wondering where the noxious stimulus is in the mandated execution scenario? The answer is: in the KCl. High levels of potassium ions excite heart muscle (so much so that it “freezes” in the excited, contracted state) and stop the heart, which is why KCl is used. But the high levels of potassium ions also excite the nociceptors, the receptors whose activation leads to a perception of pain. Think of it this way: When tissue damage occurs, cells empty their contents and those contents evoke a perception of pain. A major algesic component of cells is a high concentration of potassium ions. In sum, high concentrations of potassium ions, whether caused by an administered drug or by tissue damage, elicit a perception of pain, burning pain.
The final twist in this story came when the Oklahoma governor halted an upcoming execution because the state had used potassium acetate instead of potassium chloride. This makes no sense. None. Potassium ions are the active ingredient in the drug; the acetate or chloride is just the “carrier.” This is akin to saying that a cherry Ricola cannot substitute for a lemon Ricola. The flavoring is incidental to the cough suppression produced by the active ingredients of the Ricola. The salt (acetate or chloride) is incidental to the potassium ions delivered. However, there is a difference between the potassium compound and the Ricola candy. There must be a certain concentration of potassium ions, a certain number of potassium ion molecules has to be delivered in order to stop the heart. Since the acetate and the chloride delivery systems have different weights, a calculation is needed to figure out how much potassium acetate is needed. Understanding this calculation is one of the topics taught in the first weeks of General Chemistry at any U.S. college.
I have a very mixed reaction to these goings-on. I think that anyone that is a party to the intentional execution of people is morally compromised much in the same way that even white Americans who did not own slaves were lessened by slavery (a point beautifully made by Harriet Beecher Stowe). Because of this opinion, the end result of the potassium acetate dust-up is positive because it has had an execution-halting effect. Yet, I feel dismayed by the profoundly confused way that the positive outcome was obtained. As long as the dose of the potassium acetate is properly calculated, there is nothing wrong there (within the twisted ethical context of a state-mandated death penalty). BUT there is everything wrong with replacing a general anesthetic with an anxiolytic. My wish is to halt government-mandated killing for moral reasons. Until that goal is achieved, I hope that a bit of science can save us from the grotesqueness of killing human beings by torture.
Categories: The brain in the news




Perfect point. As a european I don’t want to enter into the debate about death penalty especially when the alternative is to be buried in a federal prison underground and not, say, in Norwegian prison that resemble more an hotel (even when you are responsible for mass killings … not kidding).
This is your country and citizen have the right to make a free choice w/o anyone from abroad to tell that you are doing it wrong.
But from a scientific POV I can express my opinion even if I am not american and say that it is umbelievable that people in charge of such responsabiity, directly or indirectly (as you exemplified with slavery), can possibly have conceived the idea of substituting a “real” sedative with an anxiolitic.
This is really really crazy. It would be the same of saying “why not using it even for standard surgery. Who cares if the patient wakes up right after the blade make the first cut”.
LikeLike
Hi Peggy,
I got your piece on drugs used for executions, and I agree with you that all legal execution is morally wrong. But the technical detail of the pharmacology was scary because it seemed to suggest that the people in charge do not know what they are doing. I am surprised they do not have well informed advisors.
I hope you are going to rerun your mooc again later this year, you have made it very hard to find any that are interesting! Almost noone has grasped the simple fact that 6-10 minute videos and lots of them, are much better for learning than the long 25 minute videos nearly everyone uses.
Anyway, my best wishes, and just to remind you that tons of your moochers found the experience really uplifting.
Mike.
LikeLike
Hi Mike,
I agree that in one way it is strange that there is no medically informed oversight. On the other hand, using “medicine” or at least pharmaceuticals to kill people runs counter to the Hippocratic oath which can includes a core proscription to do not harm.
I am going to rerun the MOOC but probably not this year. I want to put it up as open enrollment aka on-demand. That way, people can start anytime they want, take as long as they want and remain part of the learning community for as long as they want. The insight to make the videos 5-10 mins comes from Emily Bembeneck, my brilliant producer. At least I had the sense to recognize her genius and listen to all she said.
Thanks for writing and visiting my (poor neglected) blog,
P
LikeLike
Those seeking voluntary euthanasia (i.e. in terminal illness) are rebuffed, I understand, by claiming the doctor would compromise the Hippocratic Oath in abetting or aiding.
No such qualms when murdering those ‘sick’ enough to commit a crime though…
Funny too; how sickness becomes ‘framed’ as ‘badness’ and ‘evil’; depending on behaviours evinced as a result of disease, or some internal imbalance.
Having personally recently experienced close-up, the administration of a death penalty to a loved one in my arms, the sense of being party to the ending of a sentient life was profoundly distressing to me. The reasons for keeping her alive would have been selfish and to her detriment, pain, distress and increasing perplexity at diminishing mobility. The fact she was ‘only’ a dog elides the burden I will always carry as I remember her incomprehension: not being able to explain to her the ‘what’ and ‘why’.
How worthy then, for those who are able: to work towards the day when our understanding of neuroscience enables redress of a more enlightened kind.
LikeLike
Hi Gordon,
As always you have gone right for the core of the matter and have identified the piece where modern society is okay with taking a non-compassionate view. No compassion for so-called mental illness and some weird idea that mental illness is not physical or real. How or if we can ever get past that idea is not clear to me.
Watching the end of a sentient life is devastating. The first being that I ever saw die was a zebra (I was working at a zoo and the zebra had gotten very frightened by loud sounds and ran into a fence and broke its neck) and the experience profoundly affected me and altered me.
I too have held a beloved non-human (cats) as she died in my arms. However I did not experience this as a death penalty. I thought of it as a kind act, as the least that I could do for this sentient being who was no longer having a good time and whose world had grown far too confusing for comfort. I felt more taxed by my inability to explain the infirmity of my cat’s life than my inability to explain the twilight that was occurring at my request. I always felt that if we truly respected life, we would enable the same privilege to be afforded to humans.
As always, thanks for stopping by, Gordon,
P
LikeLike
“Grow old with me the best is yet to be.” She did my cat of 18 years, they tell me to multiply by 5, so she was over 90 this wonderful being that gave my life such joy. She was a force of nature stalking and chasing the deer around the yard. As for humans, if we have to kill them can we do what the vets do but with a larger dose?
Brilliant as ever, reading your book. Thanks, Peggy
LikeLike
Hello,
as always, perfect scientific article made approachable to all willing to read with comprehension!!! 🙂 Thank you for bringing insight (again) into another field.
Questions of death penalty and euthanasia are very subjective, it is about believes and opinions, there is not much that science can do towards or against it, its place is in the way of execution. My subjective opinion is that I do agree with them both. Everyone has his/hew own reasons to believe it is good or not, important is to reason well without prejudice.
LikeLike
Someone needs to forward this article to all people involved in executing prisoners.
LikeLike
A place where those in power craved information, suggestions, comments, opposing views, and even scientific inquiry would be a beautiful world.
LikeLike
Interesting piece Peggy. I’d like to pick up on the medical ethics aspect. I believe that the medical profession is failing in a broader ethical duty sense by sticking to the narrow ‘first do no harm’ principle. If there are to be executions then I believe that the medical profession have a duty to participate in that process to ensure that the process is humane, painless and effective. I am also a strong believer of the ‘right to die’ and the duty of the medical profession to assist in that process. In the latter case (unlike the execution scenario), if we believe that there is an ethical duty to respect the autonomy of the individual, we should also respect and facilitate the ultimate autonomous decision – that of terminating ones own life.
LikeLike